No Sweat — Thanks to Surgery
Published on
Children's DoctorPublished on
Children's DoctorPablo Laje, MD
Hyperhidrosis is a condition characterized by excessive sweating in certain areas of the body. The areas most commonly affected are the hands, armpits, and feet. The cause of primary hyperhidrosis is unknown. Primary hyperhidrosis affects 1% to 3% of the United States population and usually starts during childhood or adolescence.
Patients with primary hyperhidrosis have constant excessive sweating in the affected areas. The excessive sweating stops only during sleeping hours and worsens in warm environments and stressful situations. Most patients notice the excessive sweating for the first time when their moist hands begin to interfere with school and social activities. Excessive sweating in the hands can severely affect the ability to write, hold papers, use touch-screens, manipulate objects, and perform routine daily activities. It can also cause social embarrassment and impair the patient’s social interactions, which can lead to negative psychological and psychosocial consequences.
The diagnosis of primary focal hyperhidrosis is made through a thorough medical history and physical exam by the patient’s primary care provider or dermatologist.
Patients with primary hyperhidrosis are initially managed with nonsurgical treatments. The most commonly used options are:
When patients with primary hyperhidrosis do not respond to or do not tolerate nonsurgical therapies, CHOP offers a surgical treatment called thoracoscopic sympathectomy. To be a candidate for surgery, patients must undergo a thorough pre-operative workup and must have primary focal hyperhidrosis of the hands, either alone or in combination with the armpits and/or feet. Patients whose hands are not involved are not candidates for the procedure.
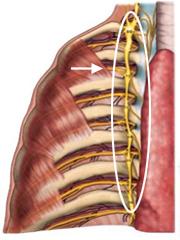 Figure A: The sympathetic chain is a nerve bundle that runs along the spine.
The sweat glands are stimulated by nerves that form a bundle called the “sympathetic chain” (see Figure A). The thoracoscopic sympathectomy is a minimally invasive surgery in which the sympathetic chain is interrupted by cutting it. The surgery requires general anesthesia, provided by our pediatric anesthesiologists. The operation is done through 2 tiny incisions in each armpit, resulting in minimal postoperative pain and nearly invisible scars (see Figure B). The whole procedure takes about 1 hour for both sides. After surgery, patients stay in the Hospital overnight for observation and go home the next morning. Patients can return to school in 2 to 3 days and resume sports in 1 week.
Figure A: The sympathetic chain is a nerve bundle that runs along the spine.
The sweat glands are stimulated by nerves that form a bundle called the “sympathetic chain” (see Figure A). The thoracoscopic sympathectomy is a minimally invasive surgery in which the sympathetic chain is interrupted by cutting it. The surgery requires general anesthesia, provided by our pediatric anesthesiologists. The operation is done through 2 tiny incisions in each armpit, resulting in minimal postoperative pain and nearly invisible scars (see Figure B). The whole procedure takes about 1 hour for both sides. After surgery, patients stay in the Hospital overnight for observation and go home the next morning. Patients can return to school in 2 to 3 days and resume sports in 1 week.
 Figure B: The operation is done through 2 tiny incisions in the armpit.
The excessive sweating of the hands is completely gone after the operation in more than 95% of patients. Patients who also have hyperhidrosis that affects the armpits and/or feet very often experience improvement in those areas as well. The surgery is more effective in children and adolescents than in adults.
Figure B: The operation is done through 2 tiny incisions in the armpit.
The excessive sweating of the hands is completely gone after the operation in more than 95% of patients. Patients who also have hyperhidrosis that affects the armpits and/or feet very often experience improvement in those areas as well. The surgery is more effective in children and adolescents than in adults.
Potential complications of the operation are pneumothorax, hemothorax, surgical site infection, and Horner’s syndrome. In experienced hands, however, the combined risk of all of them is below 1%. A potential side effect of the operation is called compensatory sweating, which is excessive sweating in areas of the body not affected prior to the operation (usually thighs or back). It is much less common in children and teenagers than in adults, and in most cases is mild.
To learn more about surgery for hyperhidrosis, contact the Division of Pediatric General, Thoracic and Fetal Surgery at 215-590-2730 or 215-590-5905. To learn more about nonsurgical options available to treat hyperhidrosis, contact the Dermatology Section at 215-590-2169.
Contributed by: Pablo Laje, MD
Categories: Surgery, Children's Doctor Winter 2015