What is an imperforate anus?
Imperforate anus, also called an anorectal malformation, is a rare birth defect that includes the absence of a normal anal opening (anus). Imperforate anus is usually diagnosed shortly after birth by a routine physical exam. The exact cause of these anal malformations is unknown.
During a bowel movement, stool passes from the large intestine to the rectum and then to the anus, where stool exits the body. Muscles in the anal area help to control when we have a bowel movement. Nerves in the area help the muscles sense the need for a bowel movement and also stimulate muscle activity.
In anorectal malformations, the anus, rectum, surrounding nerves and muscles (the lower end of the digestive tract) do not develop properly. The severity of the condition can vary greatly from child to child. There are several types of imperforate anus, each of which can affect your child’s ability to have normal bowel movements. These include:
- A membrane covering the anal opening
- Anal opening in an abnormal location
- Rectum is not connected to the anus and ends in a blind pouch
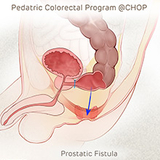
- Rectum is connected to part of the urinary tract or the reproductive system through a passage called a fistula, with no anal opening
Watch the video to learn more about our coordinated approach to caring for children with imperforate anus and other anorectal malformations.
What causes imperforate anus/anorectal malformations?
Imperforate anus is a type of anorectal malformation that affects approximately 1 in 5,000 babies. The exact cause is unknown.
How is imperforate anus diagnosed?
The diagnosis of an imperforate anus starts with a physical exam after your baby is born. Although an imperforate anus diagnosis can be made by a physical examination, physicians may recommend additional tests to identify the specific type of imperforate anus as well as evaluate for conditions associated with imperforate anus.
Children who have an imperforate anus may also have other congenital anomalies. A commonly used acronym, VACTERL, describes the associated problems that infants with imperforate anus may have:
- Vertebral defects
- Anorectal malformation
- Cardiac anomalies
- Tracheoesophageal fistula
- Esophageal atresia
- Renal (kidney) anomalies
- Limb anomalies
Diagnostic tests for evaluation of imperforate anus and associated anomalies may include:
- X-rays to help locate the degree and position of the anorectal malformation; evaluate for possible esophageal abnormalities; evaluate the bones of the spine and limbs; identify an abnormal connection of the rectum
- Ultrasound to identify associated problems of the kidneys and genitourinary tract and evaluate the spinal cord
- MRI to evaluate the pelvic anatomy and the spine
- Echocardiogram to evaluate the heart
Imperforate anus symptoms
Anorectal malformations like imperforate anus cause abnormalities in the way your child has a bowel movement. These problems will vary depending on the type of malformation.
Symptoms of imperforate anus may include the following:
- When the anal passage is narrow, your child may have a difficult time passing a bowel movement, causing constipation and possibly discomfort.
- If there is a membrane over the anal opening, your baby may be unable to have a bowel movement.
- When the rectum is not connected to the anus but there is a fistula present, stool will leave your baby's body through the fistula instead of the anus. This can cause infections.
- If the rectum is not connected to the anus and there is not a fistula present, there is no way for stool to leave the intestine. Your baby will be unable to have a bowel movement.
Imperforate anus treatment
The treatment for imperforate anus depends on the specific type of abnormality, the severity of the problem, associated anomalies, and the overall health and medical history of your child.
Children’s Hospital of Philadelphia’s Pediatric Colorectal Program offers both medical and surgical therapies for the management of imperforate anus and other anorectal malformations.
Your child will have access to a large team of specialists, including pediatric colorectal surgeons, gastroenterologists, urologists, nephrologists, neurosurgeons, nutritionists, and wound care/ostomy specialists who work together to provide comprehensive care for each patient.
Imperforate anus surgery
The majority of infants with anorectal malformations will need to have surgery to correct the problem. There are several different approaches to surgery for pediatric anorectal malformations. The specific approach and number of operations necessary depends on the complexity and type of malformation.
- A posterior sagittal anorectoplasty (PSARP) is the standard technique used for repair. This surgical method can be used when the pediatric colorectal surgeon is certain of the anatomy. PSARP repair is performed by making an incision which divides the muscles in the middle of the bottom where the new anal opening will be located. The rectum is then moved into the correct position between the muscles, and a new anus is created in the perineum. Sometimes the PSARP surgery can be performed in the newborn period.
- More commonly, the malformation is complex and a temporary colostomy will be performed, followed by imperforate anus surgery at a later date. A colostomy is an operation that diverts the path of stool to a bag which is secured to the skin. Your child is allowed to go home and grow for a few months. Your child will return to the doctor for additional X-rays to assess the location and severity of the malformation before undergoing surgery to move the rectum to the correct position and create a new anal opening. The colostomy will be reversed at a later date, often one to two months after surgery.
After surgery, the newly formed anus needs to be regularly dilated for several months. Anal dilation helps prevent narrowing of the scar tissue that could block the opening. Our Colorectal Program team will assist you with anal dilations.
Long-term outlook for children after imperforate anus surgery
Some children born with imperforate anus will end up having normal stool patterns, while others will have constipation or difficulty with incontinence. The most important predictor of long-term outlook is the severity of the imperforate anus (high or low) and the presence or absence of associated spinal and sacral abnormalities.
Children with a low lesion, especially those who require only a perineal anoplasty, may have constipation that can generally be treated with oral medications.
Children with spinal abnormalities of the lower sacrum and a high imperforate anus often do not have normal bowel continence or function. These patients are helped by a bowel management program with dietary changes, medications, and regular enemas.
Our multidisciplinary team is currently investigating the use of sacral nerve stimulators in treating fecal incontinence and constipation. This treatment involves implanting a device that delivers mild electrical pulses to the pelvic nerves and has been successful when used in conjunction with other therapies.
Toilet training children with imperforated anus
We recognize that potty-training a child with anorectal malformation can be difficult. Your child may lack the typical nerve and muscle control that is needed to control bowel movements. Our Pediatric Colorectal Program team will work with you to develop a bowel management program to help your child achieve bowel control and avoid future accidents.
Why choose Children’s Hospital of Philadelphia for imperforate anus treatment
Anorectal malformations and their associated anomalies can impact multiple areas of life, including nutrition, bowel and bladder control, kidney function, and even sexual function. Some of these issues are easily managed, but others require comprehensive care from a coordinated team.
Children’s Hospital of Philadelphia’s Pediatric Colorectal Program brings together the many specialists your child may need for their immediate treatment and long-term bowel management needs. We work closely with each family to determine the best treatment plan for your child’s unique needs that will optimize their quality of life.
We understand the challenges that come with the diagnosis of imperforate anus or anorectal malformation, and are here to support you every step of the way, from birth through adulthood. Our experience allows us to focus on every aspect of treatment, from expert surgical care to support services such as social workers who understand the unique obstacles these patients face.
Last updated: June 21, 2019

Why choose CHOP
Learn more about our experience managing the care of children with bowel management needs and how our program can help.

Your child's appointment
Learn what to expect during your child's first appointment with CHOP’s Pediatric Colorectal Program.
Resources to help

Meet your team
Here at the Pediatric Colorectal Program, you have access to a large multidisciplinary team. Experts in pediatric colorectal surgery and gastroenterology coordinate with other sub-specialists to meet your child's unique bowel management needs.
Reviewed by Myron Allukian, III, MD, Edward J. Doolin, MD, FACS, FAAP