What is laryngeal atresia?
Laryngeal atresia is a complete upper airway obstruction that occurs when the larynx fails to open during a baby's development in utero and remains blocked by cartilage or other tissue when he's born. The infant will require an immediate tracheostomy at birth in order to survive.
This condition is also called congenital high airway obstruction syndrome (CHAOS).
Testing and diagnosis
Laryngeal atresia is usually detected during prenatal ultrasound. If laryngeal atresia is suspected, the mother should be referred to the Center for Fetal Diagnosis and Treatment at CHOP for further evaluation and management.
If laryngeal atresia is not detected before birth, it presents itself immediately after delivery when the baby is unable to cry or inhale.
Treatments
Advances in fetal surgery now make it possible for babies to be operated on before they are born. One of these procedures is called a fetal EXIT (ex utero intrapartum treatment) procedure. This surgery is done in the operating room by fetal surgeons from CHOP's Center for Fetal Diagnosis and Treatment.
The EXIT procedure is not just a cesarean section. A special uterine stapling device is used to open the uterus to prevent bleeding and general anesthesia is used to preserve uteroplacental blood flow. This allows time to perform procedures such as microlaryngoscopy, bronchoscopy, tracheostomy, and surfactant administration, all of which is required to secure the airway and provide adequate ventilation. ENT surgeons from the Center for Pediatric Airway Disorders will work closely with the fetal surgeons to manage the child's airway.
Follow-up procedures
When a child with laryngeal atresia is older, he may undergo open airway reconstruction if he is shown to be a good candidate through full GI, nutrition, swallow and pulmonary evaluations.
Aero-digestive evaluation
Before an airway reconstruction can be considered, your child will need to undergo a GI evaluation by a pediatric gastroenterologist. A pediatric pulmonologist may also evaluate your child's lung status and a speech and swallowing therapist may evaluate swallow and voice. These specialists will evaluate your child and determine the need for further tests. Our surgical scheduling team will arrange a full endoscopic and GI evaluation in the operating room. This will include a microlaryngoscopy, bronchoscopy (MLB) and upper GI endoscopy (EGD), impedance probe testing and, pulmonary scopes.
During the EGD, biopsies will be taken from multiple levels up and down the aero-digestive tract and these will be screened for signs of inflammation suggestive of reflux (GERD) or food allergy inflammation (eosinophilic esophagitis). The patient is considered suitable for airway surgery when the stenosis has matured, the GERD is under control and the pulmonary status is stable. If the GERD is not under control then the patient's medication may be adjusted or changed and repeat testing will need to be done. In rare cases anti-reflux surgery may be needed.
In addition, prior to reconstructive airway surgery the child will undergo a formal feeding evaluation which includes an endoscopic evaluation of swallowing (FEES) performed in the office or a modified barium swallow. If your child does not accept food and relies exclusively on a G-tube then a flexible scope with a few drops of green dye will be used to detect pooling and aspiration. This is to make sure that your child will be able to swallow well and protect their new and enlarged airway after reconstruction. If these studies look reasonably normal then the child can undergo surgical treatment for the subglottic stenosis.
Airway reconstruction
If your child is found to be a candidate for airway reconstruction, our surgeons will perform one of two procedures:
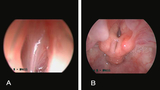
An endoscopy shows a child’s airway after it was reconstructed to treat laryngeal atresia.
References
McElhinney DB, Jacobs IN, McDonald-McGinn DM, Zackai EH, Goldmuntz E. Chromosomal and cardiovascular anomalies associated with congenital laryngeal web. Int J Pediatr Otorhinolaryngol. 2002 Oct 21;66(1):23-27.
Resources to help
Center for Pediatric Airway Disorders Resources
We have created resources to help you find answers to your questions about airway disorders and feel confident with the care you are providing your child.

Meet your team
Our coordinated approach to care, bridging many specialties at CHOP, makes it possible to meet the complex needs of children who come to us for care.