Fetal closure of a myelomeningocele (MMC) is technically more challenging than the standard postnatal closure. The access is smaller, since the surgeon must work through a small uterine window; the structures are smaller and more delicate; the placode must be handled with more care, since it is potentially functional; avoiding blood loss is critical, since a fetal transfusion is best avoided; and the surgery must be performed quickly to limit the exposure of the fetus to the extrauterine environment.
In addition, the closure must be temporarily halted if there is fetal distress or compromise of umbilical blood flow, and resumed once the issues have been resolved, necessitating constant communication between the neurosurgeon, the fetal surgeon, the maternal-fetal medicine specialist, the anesthesiologist, the fetal cardiologist and the nursing staff.
The surgery
Once the hysterotomy is accomplished with a uterine stapling device, the fetus is positioned to present the MMC defect within the hysterotomy site, and the fetus is held by a member of the fetal surgery team. The fetus should be stabilized without excessive pressure, which can lead to fetal bradycardia and diminished fetal cardiac function. The umbilical cord is located to a safe position, and the Level 1 infusion device is used to keep the fetus warm and buoyant.
A narcotic and muscle relaxant mixture is injected intramuscularly into the fetus to provide supplemental anesthesia. The skin surrounding the defect is incised to the level of the fascia with a vertical ellipse located outside of the zona epitheliosa and within full-thickness skin. The sac is mobilized circumferentially using gentle traction and a number 15 knife blade. All of the epithelialized skin is sharply excised from the placode using iris scissors, cutting into the arachnoid that surrounds the placode and releasing the connection to the sac circumferentially. After releasing the placode along with the rostral spinal cord from the sac, the tissue surrounding the placode is inspected, trimming any additional tissue that looks epidermal. Residual epithelial tissue may increase the risk of epidermoid/dermoid inclusion cyst formation. As a rule, no attempt is made to “re-neurulate” the placode. The fetal placode is quite soft and delicate, and manipulation produces trauma to potentially functional nervous tissue.
A multilayered closure is performed as in a standard postnatal closure. If present, the dura is mobilized laterally from its attachment to the underlying fascia and reflected over the placode. It is then sutured in the midline using a running 4-O Polydioxanone (PDS) stitch. In many cases, a distinct dural layer may not be large enough to provide a secure closure, and thus may have to be incorporated with the myo-fascial layer.
The skin is extensively undermined laterally by spreading with Metzenbaum scissors to allow exposure of the myo-fascial layer and to later allow for mobilization of the skin edges and skin wound closure. Small blood vessels on the surface of the fascia are coagulated with bipolar cautery. Bilateral elliptical incisions are made in the lateral myo-fascial layer, which are then undermined and reflected over the dura. Bone is included in these flaps inferiorly.
The skin is extremely thin in the fetus less than 23 weeks' gestation, requiring special care. Unlike postnatal closure, a larger, full thickness suture is needed to prevent the suture from tearing the skin. The skin is closed as a single layer with a running 4-0 PDS stitch. The closure can be aided by utilizing a “lacing” technique. The running suture is placed after tying an anchor stitch at one end, but the running stitch is left loose with the other end untied. Using a right-angle nerve hook, the sutures are gradually tightened from the anchor stitch end as forceps are used to maintain tension on the running suture. This technique dissipates the force gradually along the suture line and reduces the likelihood that the sutures will tear through the skin.
Large skin defects, especially when there is no sac (myeloschisis), cannot be closed primarily. In our institution, an elliptical shaped AlloDerm® graft is sutured to the edge of the skin defect with a continuous 4-0 PDS suture.
The hysterotomy site and maternal laparotomy are then closed by the fetal team, and the mother is stabilized and returned to her room in the immediately adjacent Special Delivery Unit at CHOP.
Surgical team needed for fetal myelomeningocele closure
- Anesthesia to administer maternal and fetal anesthesia
- Fetal cardiology to monitor fetal heart rate and function by fetal echocardiography
- Maternal-fetal medicine/obstetrics to monitor maternal and fetal health, perform fetal version when needed prior to hysterotomy, intraoperative ultrasound
- Neurosurgery to perform myelomeningocele closure
- Fetal surgery to perform hysterotomy and closure, stabilize fetus within surgical field, fetal resuscitation when needed, myelomeningocele closure, maternal laparotomy and closure
- Scrub and circulating nurses to assist with surgical procedure
- Advanced practice nurse responsible for delivery and control of the Level 1 infusion device for amniotic fluid replacement to keep the fetus warm and buoyant and to avoid umbilical cord compression
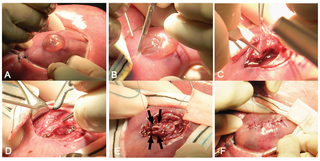
A) Stabilization of the fetal back and MMC within the hysterotomy. B) Incision in the skin surrounding the defect, outside of the zona epitheliosa and within full-thickness skin. C) Dissection of the arachnoid and residual epithelial tissue from the placode. D) Incision in the lateral myo-fascial layer and medial rotation over the placode. E) Closure of the myo-fascial layer. Note: The area containing the mobilized bone is not yet closed (black arrows). F) Closure of the skin layer.
Reference
Heuer GG, Adzick NS, Sutton LN. Fetal Myelomeningocele Closure: Technical Considerations. Fetal Diagn Ther. 2014 Aug 28. [Epub ahead of print]
Featured in this article
Specialties & Programs
Fetal closure of a myelomeningocele (MMC) is technically more challenging than the standard postnatal closure. The access is smaller, since the surgeon must work through a small uterine window; the structures are smaller and more delicate; the placode must be handled with more care, since it is potentially functional; avoiding blood loss is critical, since a fetal transfusion is best avoided; and the surgery must be performed quickly to limit the exposure of the fetus to the extrauterine environment.
In addition, the closure must be temporarily halted if there is fetal distress or compromise of umbilical blood flow, and resumed once the issues have been resolved, necessitating constant communication between the neurosurgeon, the fetal surgeon, the maternal-fetal medicine specialist, the anesthesiologist, the fetal cardiologist and the nursing staff.
The surgery
Once the hysterotomy is accomplished with a uterine stapling device, the fetus is positioned to present the MMC defect within the hysterotomy site, and the fetus is held by a member of the fetal surgery team. The fetus should be stabilized without excessive pressure, which can lead to fetal bradycardia and diminished fetal cardiac function. The umbilical cord is located to a safe position, and the Level 1 infusion device is used to keep the fetus warm and buoyant.
A narcotic and muscle relaxant mixture is injected intramuscularly into the fetus to provide supplemental anesthesia. The skin surrounding the defect is incised to the level of the fascia with a vertical ellipse located outside of the zona epitheliosa and within full-thickness skin. The sac is mobilized circumferentially using gentle traction and a number 15 knife blade. All of the epithelialized skin is sharply excised from the placode using iris scissors, cutting into the arachnoid that surrounds the placode and releasing the connection to the sac circumferentially. After releasing the placode along with the rostral spinal cord from the sac, the tissue surrounding the placode is inspected, trimming any additional tissue that looks epidermal. Residual epithelial tissue may increase the risk of epidermoid/dermoid inclusion cyst formation. As a rule, no attempt is made to “re-neurulate” the placode. The fetal placode is quite soft and delicate, and manipulation produces trauma to potentially functional nervous tissue.
A multilayered closure is performed as in a standard postnatal closure. If present, the dura is mobilized laterally from its attachment to the underlying fascia and reflected over the placode. It is then sutured in the midline using a running 4-O Polydioxanone (PDS) stitch. In many cases, a distinct dural layer may not be large enough to provide a secure closure, and thus may have to be incorporated with the myo-fascial layer.
The skin is extensively undermined laterally by spreading with Metzenbaum scissors to allow exposure of the myo-fascial layer and to later allow for mobilization of the skin edges and skin wound closure. Small blood vessels on the surface of the fascia are coagulated with bipolar cautery. Bilateral elliptical incisions are made in the lateral myo-fascial layer, which are then undermined and reflected over the dura. Bone is included in these flaps inferiorly.
The skin is extremely thin in the fetus less than 23 weeks' gestation, requiring special care. Unlike postnatal closure, a larger, full thickness suture is needed to prevent the suture from tearing the skin. The skin is closed as a single layer with a running 4-0 PDS stitch. The closure can be aided by utilizing a “lacing” technique. The running suture is placed after tying an anchor stitch at one end, but the running stitch is left loose with the other end untied. Using a right-angle nerve hook, the sutures are gradually tightened from the anchor stitch end as forceps are used to maintain tension on the running suture. This technique dissipates the force gradually along the suture line and reduces the likelihood that the sutures will tear through the skin.
Large skin defects, especially when there is no sac (myeloschisis), cannot be closed primarily. In our institution, an elliptical shaped AlloDerm® graft is sutured to the edge of the skin defect with a continuous 4-0 PDS suture.
The hysterotomy site and maternal laparotomy are then closed by the fetal team, and the mother is stabilized and returned to her room in the immediately adjacent Special Delivery Unit at CHOP.
Surgical team needed for fetal myelomeningocele closure
- Anesthesia to administer maternal and fetal anesthesia
- Fetal cardiology to monitor fetal heart rate and function by fetal echocardiography
- Maternal-fetal medicine/obstetrics to monitor maternal and fetal health, perform fetal version when needed prior to hysterotomy, intraoperative ultrasound
- Neurosurgery to perform myelomeningocele closure
- Fetal surgery to perform hysterotomy and closure, stabilize fetus within surgical field, fetal resuscitation when needed, myelomeningocele closure, maternal laparotomy and closure
- Scrub and circulating nurses to assist with surgical procedure
- Advanced practice nurse responsible for delivery and control of the Level 1 infusion device for amniotic fluid replacement to keep the fetus warm and buoyant and to avoid umbilical cord compression
A) Stabilization of the fetal back and MMC within the hysterotomy. B) Incision in the skin surrounding the defect, outside of the zona epitheliosa and within full-thickness skin. C) Dissection of the arachnoid and residual epithelial tissue from the placode. D) Incision in the lateral myo-fascial layer and medial rotation over the placode. E) Closure of the myo-fascial layer. Note: The area containing the mobilized bone is not yet closed (black arrows). F) Closure of the skin layer.
Reference
Heuer GG, Adzick NS, Sutton LN. Fetal Myelomeningocele Closure: Technical Considerations. Fetal Diagn Ther. 2014 Aug 28. [Epub ahead of print]
Contact us
Richard D. Wood Jr. Center for Fetal Diagnosis and Treatment