What is UPJ obstruction?
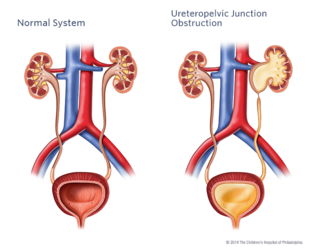
The ureteropelvic junction is located where the pelvis of the kidney meets the ureter (the tube that drains urine into the bladder). The term ureteropelvic junction (UPJ) obstruction describes a blockage to this area. The obstruction impedes the flow of urine down to the bladder, causing the urine to back up in the kidney and dilate it (hydronephrosis).
Unilateral UPJ obstruction is the most common prenatally detected obstructive disease, often picked up on maternal ultrasounds during pregnancy. Each year, the Division of Urology treats nearly 150 children who have a UPJ obstruction.
Signs and symptoms
Due to the increased use of prenatal imaging, UPJ obstruction may be identified before any symptoms are present. If any dilation (hydronephrosis) is identified, the baby will be monitored throughout the pregnancy and after birth. Once the baby is born, further imaging studies may confirm the obstruction. Older children may have back or flank pain. The pain may be associated with nausea and vomiting. Other symptoms might include bloody urine, a urinary tract infection (often with a fever), or might even be a vague abdominal pain.
Causes
UPJ obstruction usually occurs during fetal development. Most of the time, the blockage is caused when the connection between the ureter and the renal pelvis narrows. Typically in older children, UPJ obstruction can also be caused when a blood vessel is in the wrong position, crossing over the ureter and causing constriction. UPJ obstruction can also be due to scar tissue, infection, a benign polyp, or kidney stones.
Testing and diagnosis
Your child may undergo a variety of tests to help confirm his diagnosis and evaluate the extent of his condition.
- Renal bladder ultrasound (RBUS): This procedure uses sound waves to outline the kidneys and bladder. It will enable us to see the degree of hydronephrosis (dilation of the kidney).
- MAG III renal scan: This study helps us determine how each kidney is functioning and the degree of blockage. An intravenous line (IV) is used to inject a special solution called an isotope into your child's veins. The isotope makes it possible to see the kidneys clearly. Images of the kidneys will be taken with a large machine that rotates around your child. Your child will need an IV and a catheter for this study.
- MRI/MRU: MRI is a radiation-free diagnostic procedure that uses a combination of a large magnet, radiofrequencies and a computer to produce detailed images of the body. Magnetic resonance urography (MRU) creates detailed pictures of the kidneys, ureters and bladder. Your child will need an IV and a catheter for this study. Your child might need sedation if he is young and might have difficulty tolerating the length of the study, which is typically 40 minutes.
Treatment
Our overall goal in the Division of Urology in treating a UPJ obstruction is to preserve renal function. In some children, an ultrasound may show a significant amount of dilation (hydronephrosis) but the kidney functions and drains well. In this situation, we will closely follow your child with repeated imaging studies.
In situations where the kidney function is compromised, surgical intervention is needed. The surgical procedure to correct the obstruction is called a pyeloplasty. The area of obstruction in the ureter is removed and the normal area is reconnected to the kidney. Drainage tubes may be left in place to allow urine to flow across the surgical area to promote healing.
In young babies, the pyeloplasty is done through a small incision. Minimally invasive surgery (MIS) is an option for children older than 6 months. The pyeloplasty can be done either laparoscopically or through a robotic assisted laparoscopic approach. The minimally invasive approach is accomplished through three small incisions, the size of a grain of rice. The advantages are smaller, less visible incisions and a quicker recovery period. The minimally invasive technique is not appropriate for all children. Your healthcare provider will work with you and your family to determine what kind of intervention is best.
Reviewed by: Division of Urology
Date: May 2011
Resources to help
Division of Urology Resources
Caring for a child with an illness or injury can be overwhelming. We have resources to help you find answers to your questions and feel confident in the care you are providing your child.

Meet your team
At CHOP, your child's care is in the hands of one of the largest and most accomplished teams of pediatric urology experts in the world.