
Case: A 4-year-old boy presented to the emergency room reporting 2 weeks of right knee pain, swelling, and limping. He had elevated inflammatory markers, and his right knee was swollen, warm, and tender. Due to concern for septic arthritis, the knee was aspirated and antibiotics were started. The knee failed to improve, which prompted a synovial biopsy, approximately 2 months after presentation to ER. Biopsy revealed acute and chronic inflammation. The patient was referred to Rheumatology. At his first exam with Rheumatology, abnormalities were noted in the patient’s eyes, particularly “white coating” on cornea and poorly reactive pupils.
The patient was sent for immediate evaluation by Ophthalmology. Both eyes had active anterior uveitis, bilateral posterior synechiae (iris scarring to the lens), and band keratopathy. His vision was reduced to 20/70 right eye and 20/200 left eye. Optic nerve and macular edema were present as well.
Because of his vision-threatening uveitis, he was admitted to the hospital to receive intravenous steroids and anti-TNF-alpha treatment (infliximab). He continued on monthly infliximab and weekly methotrexate. His vision has improved to 20/25 right eye and 20/50 left eye. His arthritis has resolved, and he is fully active. He will require surgery to remove the band keratopathy and improve vision.
Discussion: The diagnosis of anterior uveitis is made with slit lamp exam by an ophthalmologist, but in advanced and severe cases ophthalmic findings can be visible on gross exam to non-ophthalmologists by penlight or direct ophthalmoscopy.
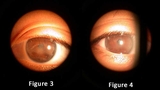
Anterior uveitis is inflammation in the anterior chamber of the eye, representing inflammation of the iris and ciliary body. Band keratopathy is deposition of calcium in the anterior cornea. Band keratopathy will begin at the nasal and temporal cornea, but if inflammation is not controlled it can extend more centrally into the visual axis (as in this patient). Synechiae represent adhesion between the iris and the lens and can cause the pupil to be misshapen, small, or poorly reactive, and can result in elevated intraocular pressure. (See Figures 3 and 4.) Cataracts and glaucoma are other complications of uveitis that can cause vision loss. The key to preventing complications and vision loss from uveitis is early diagnosis and adequate control of the disease once the diagnosis is made.
As juvenile idiopathic arthritis (JIA) is the most common rheumatic disease in children, it should be considered in any child under 16 years who presents with a persistently swollen joint. About 13% of children with JIA will develop chronic anterior uveitis. The risk of anterior uveitis is higher (up to 30%) in children with the oligoarticular sub-type of JIA. In oligoarticular JIA, 4 or fewer joints are affected, usually larger joints (knees, ankles, wrists) in the first 6 months of disease.
The uveitis associated with JIA is most commonly asymptomatic, whereas other types of uveitis cause redness, pain, and light sensitivity. Patients who are newly diagnosed with JIA require a baseline, then frequent ophthalmic exams, to catch the silent uveitis if it appears. Screening frequency is highest in those with younger age of onset, shorter disease duration, oligoarticular/psoriatic/polyarticular subtypes, and ANA positivity (ANA IFA).
Initial treatment of uveitis involves topical steroids (eyedrops) to reduce acute inflammation. Unfortunately, the ocular complications of steroid use include cataracts and glaucoma, similar to the complications of uveitis itself. In chronic, recurrent, or severe cases, systemic steroid sparing agents are necessary to control inflammation and improve visual outcomes by reducing disease associated and steroid caused complications. Methotrexate successfully controls uveitis in about two-thirds of patients. TNF-alpha inhibition additionally controls another three-quarters of patients. Other biologics may be used in recalcitrant disease.
Because of the intersection of severe complications to both joints and eyes, it is essential that the divisions of Rheumatology and Ophthalmology communicate regularly to best manage these complex patients. To this end, in 2013, Children’s Hospital of Philadelphia created the Uveitis Coordinated Care Clinic. This clinic partners a rheumatologist and ophthalmologist who see patients together in the same clinical space. This arrangement allows for collaborative discussions with parents and each specialist, facilitating more efficient and informed clinical decision making. In addition, patients and their parents appreciate missing less work and school by seeing 2 specialists on the same day.
Featured in this article
Specialties & Programs
Case: A 4-year-old boy presented to the emergency room reporting 2 weeks of right knee pain, swelling, and limping. He had elevated inflammatory markers, and his right knee was swollen, warm, and tender. Due to concern for septic arthritis, the knee was aspirated and antibiotics were started. The knee failed to improve, which prompted a synovial biopsy, approximately 2 months after presentation to ER. Biopsy revealed acute and chronic inflammation. The patient was referred to Rheumatology. At his first exam with Rheumatology, abnormalities were noted in the patient’s eyes, particularly “white coating” on cornea and poorly reactive pupils.
The patient was sent for immediate evaluation by Ophthalmology. Both eyes had active anterior uveitis, bilateral posterior synechiae (iris scarring to the lens), and band keratopathy. His vision was reduced to 20/70 right eye and 20/200 left eye. Optic nerve and macular edema were present as well.
Because of his vision-threatening uveitis, he was admitted to the hospital to receive intravenous steroids and anti-TNF-alpha treatment (infliximab). He continued on monthly infliximab and weekly methotrexate. His vision has improved to 20/25 right eye and 20/50 left eye. His arthritis has resolved, and he is fully active. He will require surgery to remove the band keratopathy and improve vision.
Discussion: The diagnosis of anterior uveitis is made with slit lamp exam by an ophthalmologist, but in advanced and severe cases ophthalmic findings can be visible on gross exam to non-ophthalmologists by penlight or direct ophthalmoscopy.
Anterior uveitis is inflammation in the anterior chamber of the eye, representing inflammation of the iris and ciliary body. Band keratopathy is deposition of calcium in the anterior cornea. Band keratopathy will begin at the nasal and temporal cornea, but if inflammation is not controlled it can extend more centrally into the visual axis (as in this patient). Synechiae represent adhesion between the iris and the lens and can cause the pupil to be misshapen, small, or poorly reactive, and can result in elevated intraocular pressure. (See Figures 3 and 4.) Cataracts and glaucoma are other complications of uveitis that can cause vision loss. The key to preventing complications and vision loss from uveitis is early diagnosis and adequate control of the disease once the diagnosis is made.
As juvenile idiopathic arthritis (JIA) is the most common rheumatic disease in children, it should be considered in any child under 16 years who presents with a persistently swollen joint. About 13% of children with JIA will develop chronic anterior uveitis. The risk of anterior uveitis is higher (up to 30%) in children with the oligoarticular sub-type of JIA. In oligoarticular JIA, 4 or fewer joints are affected, usually larger joints (knees, ankles, wrists) in the first 6 months of disease.
The uveitis associated with JIA is most commonly asymptomatic, whereas other types of uveitis cause redness, pain, and light sensitivity. Patients who are newly diagnosed with JIA require a baseline, then frequent ophthalmic exams, to catch the silent uveitis if it appears. Screening frequency is highest in those with younger age of onset, shorter disease duration, oligoarticular/psoriatic/polyarticular subtypes, and ANA positivity (ANA IFA).
Initial treatment of uveitis involves topical steroids (eyedrops) to reduce acute inflammation. Unfortunately, the ocular complications of steroid use include cataracts and glaucoma, similar to the complications of uveitis itself. In chronic, recurrent, or severe cases, systemic steroid sparing agents are necessary to control inflammation and improve visual outcomes by reducing disease associated and steroid caused complications. Methotrexate successfully controls uveitis in about two-thirds of patients. TNF-alpha inhibition additionally controls another three-quarters of patients. Other biologics may be used in recalcitrant disease.
Because of the intersection of severe complications to both joints and eyes, it is essential that the divisions of Rheumatology and Ophthalmology communicate regularly to best manage these complex patients. To this end, in 2013, Children’s Hospital of Philadelphia created the Uveitis Coordinated Care Clinic. This clinic partners a rheumatologist and ophthalmologist who see patients together in the same clinical space. This arrangement allows for collaborative discussions with parents and each specialist, facilitating more efficient and informed clinical decision making. In addition, patients and their parents appreciate missing less work and school by seeing 2 specialists on the same day.
Contact us
Division of Ophthalmology