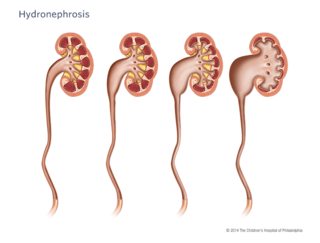
What is hydronephrosis?
When urine can’t drain properly from your child’s kidney to their bladder, their kidney can become enlarged (dilated) with that extra urine. This is called “hydronephrosis,” or you might also hear your doctor call it, “urinary tract dilation.”
Hydronephrosis can range from mild to severe, depending on the cause of the dilation. Often children who have hydronephrosis have it from the time of birth.
How is hydronephrosis diagnosed?
Prenatal hydronephrosis (which may also be called antenatal hydronephrosis, or fetal urinary tract dilation) is one of the most common fetal anomalies diagnosed before birth.
Due to the increased use of prenatal ultrasound, we’re able to detect hydronephrosis sooner than we were able to in the past. Hydronephrosis is now found in 1 out of 100 pregnancies.
If hydronephrosis is detected, you’ll have more follow-up ultrasounds to monitor amniotic fluid levels, the amount of dilation, if the dilation is in one of your child’s kidneys or both, if their ureters are dilated, and if there is normal filling and emptying of their bladder. If your provider chooses, they may refer you to our Richard D. Wood Jr. Center for Fetal Diagnosis and Treatment for more in-depth imaging and discussion.
Causes of hydronephrosis
- Vesicoureteral reflux (VUR). VUR is a condition in which urine travels backward from the bladder up towards the kidney. This may affect one or both ureters (the tubes that normally carry urine from the kidney to the bladder).
- Obstruction or blockage. An obstruction can occur at any location along the urinary tract:
- The ureteropelvic junction (UPJ), where the ureter is connected to the kidney
- The ureterovesical junction (UVJ) where the ureter enters the bladder; this can be an intrinsic narrowing, or may be associated with ureterocele, which is a balloon-like obstruction at the end of the ureter
- In the urethra in boys (posterior urethral valve, PUV)
- No significant abnormality. The dilation in many of these kidneys eventually resolves over time and no specific cause is discovered.
Signs and symptoms of hydronephrosis
Many children with hydronephrosis or urinary tract dilation may not have any symptoms. About 75% of hydronephrosis detected before birth will resolve on its own.
In more severe cases of hydronephrosis, some babies will not have any symptoms, while other children may experience acute kidney pain, bleeding or urinary tract infections, depending on the underlying cause.
Testing and diagnosis of hydronephrosis
Prenatal testing
Sonogram
Hydronephrosis can be detected on an ultrasound as early as the first trimester of pregnancy and is typically seen on the anatomy ultrasound around 20 weeks’ gestation.
In most cases, if your child is diagnosed with hydronephrosis before birth, you’ll receive follow-up ultrasounds for the remainder of your pregnancy to track your child’s kidney health.
Postnatal testing
Renal bladder ultrasound (RBUS)
A renal bladder ultrasound uses sound waves to outline the kidneys and bladder. It will enable us to see the degree of your child’s hydronephrosis.
Images from the ultrasound are used to evaluate the size and appearance of their “collecting system” (which is made up of the renal pelvis and calyces), and the appearance of their renal parenchyma, ureter and bladder.
Voiding cystourethrogram (VCUG)
In a voiding cystourethrogram (VCUG), a tube (catheter) is placed through your child’s urethra and into their bladder. The tube will be used to slowly fill the bladder with a contrast solution and pictures will be taken.
While the bladder is being filled, a special machine (fluoroscopy) is used to take pictures. If special ultrasound contrast is used, these pictures can be taken with an ultrasound machine (this is called a contrast-enhanced voiding cystourethrogram or CeVUS). The radiologist looks to see if any of the solution is going back up into the kidneys. This study confirms the diagnosis of vesicoureteral reflux.
Additional pictures are taken while your child is urinating. The radiologist will look at the urethra while urine is passing to be sure there is no blockage (PUV, or improper contraction of the urethral sphincter).
MAG III renal scan
A MAG III renal scan may be performed to determine how each of your child’s kidneys are functioning and how well each kidney drains into their ureter and down into the bladder. An intravenous line (IV) is used to inject a special solution called an isotope into their veins. The isotope is processed by the kidney so that it can show how well the kidney works. A tube (catheter) will also be placed into your child’s bladder to make sure the bladder is able to empty completely. Pictures of the kidneys will be taken with a large X-ray machine that rotates around your child.
MRI/MRU
MRI is a radiation-free diagnostic procedure that uses a combination of a large magnet, radiofrequencies and a computer to produce detailed images of the body.
Magnetic resonance urography (MRU) also requires an intravenous line (IV) to inject a contrast called gadolinium, and a tube (catheter) will also be placed into your child’s bladder. The contrast is processed by the kidney so that the MRI can capture very detailed pictures of their kidneys, ureters and bladder. This study helps us understand how well their kidney's function and drain, as well as showing their anatomy very clearly.
Hydronephrosis treatment
Our team in the Division of Urology will take a thorough history, review any imaging with you, and tailor a hydronephrosis treatment plan based on your child’s individual needs.
Treatment for hydronephrosis depends on several factors, including the cause of the hydronephrosis, if it is causing any symptoms (pain, infection), or if the hydronephrosis may be causing any damage to the kidney over time.
Treatment may include:
- Close observation with periodic ultrasound to make sure the dilation in the kidney goes away
- Use of a low dose of antibiotic once a day to prevent urinary tract infection
- Surgery to relieve obstruction or correct vesicoureteral reflux
Every child is different, and so each treatment plan is tailored to your child’s specific needs.
Resources for clinicians
This clinical pathway can be used to guide the evaluation and management of patients presenting with ultrasound findings of perinatal urinary tract dilation (UTD). This pathway should be used by pediatricians, neonatologists, and urologists to guide risk-based evaluation and treatment based on pre-natal and post-natal ultrasound findings.
Review the pathway: Evaluation and Management of Neonates Presenting with Findings of Perinatal Urinary Tract Dilation.
Resources to help
Division of Urology Resources
Caring for a child with an illness or injury can be overwhelming. We have resources to help you find answers to your questions and feel confident in the care you are providing your child.

Meet your team
At CHOP, your child's care is in the hands of one of the largest and most accomplished teams of pediatric urology experts in the world.
Patient stories

Reviewed by Dana A. Weiss, MD, Jennifer Kirk, BSN, MSN, CPNP
Reviewed on 04/25/2025