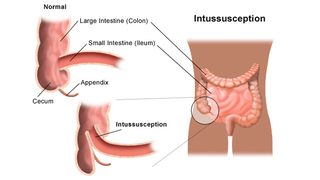
What is intussusception?
Intussusception is a life-threatening illness and occurs when a portion of the intestine folds like a telescope, with one segment slipping inside another segment. This causes an obstruction, preventing the passage of food that is being digested through the intestine.
If left untreated, it can cause serious damage to the intestines, intestinal infection, internal bleeding and a severe abdominal infection called peritonitis.
Intussusception is the most common cause of intestinal obstruction in children between the ages of three months and six years.
Causes of intussusception
The cause of intussusception is not known, although viral infections may be responsible in some cases. It may be caused by an abnormality (such as a polyp) in the intestines or as a result of recent intestinal surgery.
In most children there is no abnormality present, and the cause is unknown.
Sixty percent of those who develop intussusception are between 2 months and 1 year of age. Intussusception is rarely seen in newborn infants.
Boys develop intussusception four times more often than girls.
Although 80 percent of the children who develop the condition are less than 2 years old, intussusception can also occur in older children, teenagers and adults.
Intussusception and the rotavirus vaccine
Learn more about rotavirus vaccines and intussusception from the Vaccine Education Center at CHOP.
Symptoms of intussusception
The most common symptom of intussusception is sudden onset of intermittent pain in a previously well child. However, each child may experience symptoms differently. The pain may be mistaken for colic at first, and occurs at frequent intervals.
Infants and children may strain, draw their knees up, act very irritable and cry loudly. Your child may recover and become playful between bouts of pain, or may become tired and weak from crying.
Vomiting may also occur with intussusception, and usually starts soon after the pain begins.
Your child may pass a normal stool, but the next stool may look bloody. Further, a red, mucus or jelly-like stool is usually seen with intussusception.
Physical examination may reveal a “sausage-shaped” mass felt upon palpation of the abdomen.
Symptoms of intussusception may resemble other conditions or medical problems. Please consult a physician for a diagnosis.
Diagnosis
If your child is in abdominal pain, call your doctor for an appointment as soon as possible. If your child cannot be seen soon, go to the Emergency Department to be evaluated.
A physician will obtain your child’s medical history and perform a physical examination to determine if they have intussusception.
Imaging studies are also done to examine the abdominal organ and aid in making an accurate diagnosis of your child. These tests may include:
- Abdominal X-ray: This diagnostic test may show the intestinal obstruction. A radiologist may see an increased density of the telescoped bowel or other sights indicative of bowel obstruction.
- Ultrasound: This radiologic test of choice uses sound waves to create pictures of the inside of the body. On ultrasound, a target-like sign can be seen that is indicative of intussusception.
- Air or contrast enema: This procedure can be diagnostic, and in some cases serve as the treatment for intussusception. Air or a contrast fluid is given into the rectum as an enema. An X-ray of the abdomen shows narrow areas, blockages and other issues. On some occasions, the pressure exerted on the intestine while inserting air or contrast will help the intestine to unfold, correcting the intussusception.
Treatment for intussusception
Intussusception is not usually immediately life-threatening. It can be treated with either a water-soluble contrast enema or an air-contrast enema, which both confirms the diagnosis of an intussusception, and in most cases successfully reduces it.
Enema
An enema is done by placing a small tube into the rectum. Fluid or air is gradually added into the tube to allow clinicians to see the intussusception that is blocking the intestine via X-ray or ultrasound.
The pressure of the fluid or air pushes the telescoping bowel back to its normal position, fixing the problem.
There is a chance the intussusception can recur within 24 hours. Children should be monitored for symptoms once discharged from the hospital.
Most of the time the enema will take care of the bowel problem. However, in 10-15 percent of cases, the bowel cannot be reduced and surgery is necessary.
Surgery
In a reduction of the bowel surgery, the surgeon may choose to do the procedure with one larger incision (called an open procedure) or laparoscopically, with tiny incisions and a camera. The surgical procedure used will depend on your child’s condition.
Whether open surgery or laparoscopic, the intussusception is carefully reduced by gently pushing the leading portion of the intussusceptions back upstream to reduce the telescoping of the bowel.
If the surgeon is unable to successfully reduce the bowel, then the afflicted section will need to be removed. When this happens, the surgeon must remove the affected part of the intestine and sew the two healthy sections back together.
The intestines will be stitched with sutures that dissolve. The outside skin is usually closed with stitches that will dissolve and then covered with gauze and/or a clear dressing.
Follow-up care after treatment
Enema
If your child received an enema, the air will pass out of the intestines. The gas may persist for a few hours after the test. It is normal during this time to have a fever and your child may be given Tylenol (acetaminophen) to bring down the fever.
Following the enema, your child will slowly be allowed to start drinking and eating.
Once your child is eating and feeling better, you will be able to take them home. We ask you bring your child back to the hospital if any symptoms return.
Surgery for intussusception
If your child had surgery to treat intussusception, they will recover in the post-acute care unit for an hour or so, and then will be moved to a hospital room.
Your child may experience pain and will receive medication through an IV if needed. It is also normal to have a fever during this time, so Tylenol (acetaminophen) may also be used to reduce the fever.
Your child’s incision may have a clear (derma bond) dressing or a gauze dressing. The clear dressing will dissolve. Gauze dressings are removed two days after surgery.
After surgery, your child may have small sips of clear liquids. If your child drinks fluids and does not vomit, we will allow them to slowly start eating again. Once your child is eating and feeling better, you will be able to take your child home. Your child may bathe or shower on the second day after surgery.
We will work with you to schedule a follow-up appointment with your child's surgeon 2-3 weeks after discharge. Your child may not participate in contact sports or gym until after the follow-up visit with the surgeon.
When to call the doctor
After your child has been treated for intussusception, it is important that you carefully monitor your child’s health. Call the doctor if your child experiences any of the following symptoms:
- Fever greater than 101 degrees
- Any sign of infection, including: redness, swelling, warmth, yellow/green drainage from incision or tenderness. This is particularly important for children who have had surgery.
- Vomiting
- Diarrhea or jelly-like stools
- Episodic, cramps and abdominal pain
- Any questions or concerns
If your child suffers any of the signs or symptoms described above, they must be brought to the Emergency Department as quickly as possible to receive proper treatment.

Why choose CHOP for your child's surgery
If your child needs surgery, you want to know their care is in the hands of the best, most compassionate team. CHOP's world-class pediatric surgeons and experienced staff are here for you.

Preparing for surgery
Find tips to prepare for your preoperative visit with CHOP’s pediatric general surgeons, and resources to help prepare your child for surgery.
Resources to help
Division of Pediatric General, Thoracic and Fetal Surgery Resources
We have created resources to help you find answers to your questions and feel confident with the care you are providing your child.

Meet your team
Here at the Division of General, Thoracic and Fetal Surgery, you have access to world-class pediatric surgeons who are experts in meeting children’s unique surgical needs. Our surgical team is extensive.