What is sacrococcygeal teratoma (SCT)?
Sacrococcygeal teratoma (SCT) is a tumor. It develops before a baby is born and grows from the baby’s tailbone (also called the coccyx). An SCT is the most common congenital tumor, which means it is present at birth. SCT occurs in as many as 1 in 10,000 births. Female fetuses are four times more likely to develop an SCT than males. Most fetal sacrococcygeal teratomas are not malignant, meaning they are not cancerous.

There are different types of sacrococcygeal tumors. The type depends on their location and severity.
- Type I SCT tumors: Almost completely external (outside the body) and attached to the baby’s tailbone.
- Type II SCT tumors: Mostly external with a small (but significant) part of the tumor growing inside the body.
- Type III SCT tumors: Visible externally but with the tumor growing in the pelvis and extending into the abdomen.
- Type IV SCT tumors: Completely internal.
Sacrococcygeal tumors also vary in their appearance:
- Cystic SCT: Contains clusters of fluid-filled areas with few blood vessels.
- Solid SCT: Dense tumors containing many blood vessels.
- Mixed SCT: Contain both cystic and solid areas.
The outcome for a baby diagnosed with SCT varies depending on the size, location, and type of tumor. Some SCTs can be life-threatening if they are not treated. This is why early and accurate diagnosis is important. En Español »
What causes sacrococcygeal teratoma?
The causes of sacrococcygeal teratoma are not known. The tumor grows from germ cells. Germ cells are the cells that develop into the embryo and make up the reproductive system of men and women.
Signs and symptoms of sacrococcygeal teratoma
Sacrococcygeal teratomas are usually discovered during a routine prenatal ultrasound. The ultrasound technologist may notice a mass of tissue. This mass may be growing from the baby’s tailbone and/or inside the baby’s abdomen.
Some babies can show symptoms from the SCT such as fluid accumulation in the chest, abdomen, scalp or skin. This is called fetal hydrops. If this develops during your pregnancy, an urgent evaluation at a high-volume fetal center is necessary given the risks of fetal loss and maternal mirror syndrome. Mirror syndrome is a condition when the mom also collects fluid in her body. It can lead to dangerously high blood pressure and other problems.
Evaluation and diagnosis of sacrococcygeal teratoma
Our team at the Richard D. Wood Jr. Center for Fetal Diagnosis and Treatment (CFDT) is here for you. If you turn to us for care, you will first speak with a knowledgeable fetal therapy nurse coordinator or genetic counselor. They will answer your questions and schedule a comprehensive one-day evaluation.

Our team has seen more than 386 patients with SCT. This unique level of experience makes us one of the few teams qualified to manage your baby’s condition.
We have a team of dedicated imaging specialists. They use the most advanced prenatal imaging techniques and state-of-the-art technologies available. This allows them to gather detailed information about your baby’s diagnosis.
- High resolution fetal ultrasound allows us to study the SCT and fetal anatomy and determine fetal well-being.
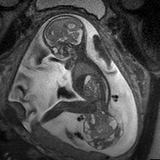
- Ultrafast fetal MRI is a technique pioneered at Children’s Hospital of Philadelphia. It allows us to see even more detail about the SCT and determine if it could be invading the region of the spine.
- Fetal echocardiogram lets us study the structure and function of the heart.
These specialized tests help us determine the type, size and location of the SCT. They also allow us to:
- Check the placenta
- Measure the amount of amniotic fluid around the baby
- Determine any impact on the baby’s heart that may cause hydrops (fluid accumulation)
- Determine the level of risk involved to the ongoing pregnancy. We do this by calculating the ratio between the tumor volume and the baby’s weight (how big the tumor is compared to how big the baby is) when the fetus is less than 24 weeks.
Management of SCT during pregnancy
After all testing is complete, our team meets with you and your family. This meeting will include a maternal-fetal medicine (MFM) specialist and a pediatric surgeon. Both have experience managing pregnancies affected by SCT.
Together, they will:
- Review the imaging results
- Discuss the diagnosis
- Explain treatment options and potential outcomes
- Answer any questions you may have
You will return to our Center for frequent follow-up ultrasounds and prenatal care. We determine the frequency of follow-up appointments based on your specific pregnancy needs. After each ultrasound, you will meet with an MFM who will update you on the baby.
Our outpatient team of nurse practitioners and nurse midwives provides your prenatal care. They will collaborate with the MFMs. Discussions about delivery planning will be ongoing. This is because babies with SCT are often delivered early. This is especially true if tumor growth ramps up or the baby develops signs of hydrops.
Sacrococcygeal teratoma treatment
Treatment for SCT involves surgery to remove the tumor. Timing of treatment depends on the diagnosis and severity of your child’s tumor. They may undergo fetal surgery to remove the SCT before birth, or they may have tumor resection surgery after they're born.
Determining severity of SCT before delivery
Some SCTs are fluid-filled (cystic), with few blood vessels. These are generally well tolerated during pregnancy, regardless of their location.
Large tumors that are solid and have many blood vessels can be a risk to the baby and the pregnancy. The baby’s heart has to pump blood to support its body and the blood vessels in the tumor. This makes the heart work much harder than normal. If the fetus’s heart can’t keep up with the demand, fetal hydrops (fluid accumulation) may develop.
Hydrops can cause heart failure in the fetus. Hydrops can also impact the mother's health. The mother may “mirror” symptoms of the baby. This can include swelling and blood pressure changes. These changes call for immediate assessment and care.
Because of these risks, we follow fetuses with large, solid SCTs that have many blood vessels very closely.
Fetal intervention for sacrococcygeal teratoma
Some SCTs are large, solid, have significant blood flow, and are external. In these cases, there is the possibility of removing all or part of the tumor before the baby is born.
We call this maternal-fetal surgery to remove a fetal SCT. It involves a team of highly skilled fetal surgeons and maternal-fetal medicine specialists. They open the mother’s abdomen and uterus to remove as much of the SCT from the baby’s tailbone as they can. After surgery, we follow the pregnancy until the time of delivery.
Delivery of babies with SCT and surgery after birth
The type, size and location of the SCT helps guide the timing and type of delivery for your baby. Delivery will occur in our Garbose Family Special Delivery Unit (SDU). This is the world's first birth facility of its kind. It is for healthy mothers carrying babies with birth defects.
Sometimes, we can do a vaginal delivery. Other cases call for a more specialized approach to delivery.
- Cesarean delivery (C-section) to immediate neonatal resection – This is when we deliver a baby by C-section. Then they have immediate surgery in an adjoining room to remove the tumor.
- EXIT to neonatal resection – This is a specialized procedure. During C-section delivery, the baby stays attached to the placenta. They continue receiving oxygen through the umbilical cord while the pediatric surgeon removes as much of the tumor as they can. After surgery, we complete the delivery and bring the baby to the Newborn/Infant Intensive Care Unit (N/IICU).
The time right after a baby with a birth defect is born is critical. These newborns can face a lot of challenges. Transitioning from the mother’s womb to the world can be difficult. They need expert delivery room support.
At Children’s Hospital of Philadelphia (CHOP), we have a unique Newborn Stabilization and Resuscitation Team. This team has the skills to care for high-risk babies born with known birth defects. They use cutting-edge monitoring and technology. This allows them to check every aspect of a baby’s health immediately after birth.
Babies who need surgery immediately or soon after birth are in the best hands, from the very start. Our Neonatal Surgical Team provides the vital care your baby needs from the moment they arrive to the N/IICU and throughout their hospitalization.
N/IICU stay for babies with sacrococcygeal teratoma
Length of stay in the N/IICU varies depending on the gestational age at delivery (how many weeks the mother was into the pregnancy when the baby was born) and surgical needs of the baby. Parents are a vital part of the baby’s team. You will have 24-hour access to your baby during their N/IICU stay. We encourage your presence and interaction with your baby as much as possible.
Follow-up care for babies born with SCT
Babies born with an SCT may need follow-up care for bladder or bowel concerns. We will make your first appointments with specialists before your baby leaves the N/IICU. Your baby will also have regular follow-up with their pediatric surgeon and pediatrician.
Long-term outlook
The sacrococcygeal teratoma survival rate is very high. Most fetal sacrococcygeal teratomas are not likely to be cancerous (malignant). The prognosis tends to be good after removal of the tumor, but ongoing follow-up is needed for the first three years of life.

Tour our Fetal Center
The Wood Center for Fetal Diagnosis and Treatment has cared for many families and will help you through your journey, too.

What to expect
From the moment of referral through delivery and postnatal care, your family can expect a supportive experience when you come to us with a diagnosis of a birth defect.
Resources to help
Sacrococcygeal Teratoma (SCT) Resources
Richard D. Wood Jr. Center for Fetal Diagnosis and Treatment Resources
Learning your baby has a birth defect is a life-changing experience. We want you to know that you are not alone. To help you find answers to your questions, we've created this list of educational health resources.

Meet your team
You will receive care from a highly skilled and compassionate team with a global reputation. This team helped shape modern fetal care and continues to improve techniques and treatments.
Patient stories

