
Case
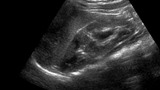
An 18-month-old girl returns for a follow-up appointment with her urologist. She has a history of grade 3 vesicoureteral reflux (VUR) into the lower pole of a duplex left kidney identified at 4 months of age following febrile urinary tract infections (UTI) (See Figure 1). She is healthy, takes prophylactic antibiotics and has not experienced additional UTIs. Her growth and development are normal. To guide her further care, a newer type of ultrasound, a contrast-enhanced voiding urosonography, would be the most appropriate imaging study.
Discussion
The growth and development of her kidneys and status of her VUR will help direct her urological care going forward. This assessment had routinely been accomplished through a renal bladder ultrasound (US) and voiding cystourethrogram (VCUG).
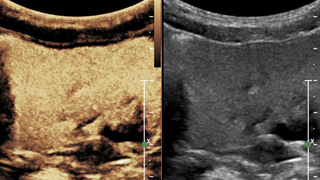
An alternative examination is contrast-enhanced voiding urosonography (ceVUS), during which an ultrasound contrast agent is instilled into the urinary bladder and ultrasound is used to assess the urinary tract and grade VUR in a similar fashion to VCUG.
US contrast agents are microbubbles, which are smaller than red blood cells, comprised of an inert gas and stabilized by a lipid or protein shell. The microbubbles oscillate when imaged with US and, through US machine software, their signal can be distinguished from other tissues. The US contrast agents have been proven to be safe when instilled in the urinary system. While pediatric contrast-enhanced US has been performed since the early 1990s outside of the United States, it was not until the 2016, when the U.S. Food and Drug Administration (FDA) approved an ultrasound contrast agent for ceVUS in children, that the exam became more commonly offered.
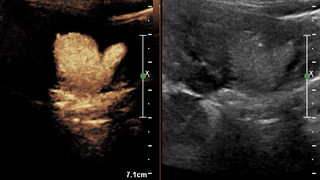
While ceVUS requires bladder catheterization similar to VCUG, it has a number of advantages including: no ionizing radiation, the child remains in close proximity to their caregiver, US equipment is smaller and less intimidating, the child can void in the upright position, and ceVUS detects more VUR and higher grades of reflux compared to VCUG. It is performed in the US department following grayscale imaging of the kidneys and bladder.
ceVUS was first offered as a clinical examination at Children’s Hospital of Philadelphia in 2014 and now is increasingly replacing VCUGs in CHOP’s Department of Radiology.
References and Further Readings
Darge K. Voiding urosonography with ultrasound contrast agents for the diagnosis of vesicoureteric reflux in children. I. Procedure. Pediatr Radiol. 2008;38(1):40-53.
Darge K, Troeger, J. Vesicoureteral reflux grading in contrast-enhanced voiding urosonography. Eur J Radiol. 2002;43(2):122-128.
Papadopoulou F, Ntoulia A, Siomou E, Darge K. Contrast-enhanced voiding urosonography with intravesical administration of a second-generation ultrasound contrast agent for diagnosis of vesicoureteral reflux: prospective evaluation of contrast safety in 1 010 children. Pediatr Radiol. 2014;44(6):719-28.
Darge K. Voiding urosonography with US contrast agents for the diagnosis of vesicoureteric reflux in children. II. Comparison with radiological examinations. Pediatr Radiol. 2008;38(1):54-63; quiz 126-127.
Featured in this article
Specialties & Programs
Case
An 18-month-old girl returns for a follow-up appointment with her urologist. She has a history of grade 3 vesicoureteral reflux (VUR) into the lower pole of a duplex left kidney identified at 4 months of age following febrile urinary tract infections (UTI) (See Figure 1). She is healthy, takes prophylactic antibiotics and has not experienced additional UTIs. Her growth and development are normal. To guide her further care, a newer type of ultrasound, a contrast-enhanced voiding urosonography, would be the most appropriate imaging study.
Discussion
The growth and development of her kidneys and status of her VUR will help direct her urological care going forward. This assessment had routinely been accomplished through a renal bladder ultrasound (US) and voiding cystourethrogram (VCUG).
An alternative examination is contrast-enhanced voiding urosonography (ceVUS), during which an ultrasound contrast agent is instilled into the urinary bladder and ultrasound is used to assess the urinary tract and grade VUR in a similar fashion to VCUG.
US contrast agents are microbubbles, which are smaller than red blood cells, comprised of an inert gas and stabilized by a lipid or protein shell. The microbubbles oscillate when imaged with US and, through US machine software, their signal can be distinguished from other tissues. The US contrast agents have been proven to be safe when instilled in the urinary system. While pediatric contrast-enhanced US has been performed since the early 1990s outside of the United States, it was not until the 2016, when the U.S. Food and Drug Administration (FDA) approved an ultrasound contrast agent for ceVUS in children, that the exam became more commonly offered.
While ceVUS requires bladder catheterization similar to VCUG, it has a number of advantages including: no ionizing radiation, the child remains in close proximity to their caregiver, US equipment is smaller and less intimidating, the child can void in the upright position, and ceVUS detects more VUR and higher grades of reflux compared to VCUG. It is performed in the US department following grayscale imaging of the kidneys and bladder.
ceVUS was first offered as a clinical examination at Children’s Hospital of Philadelphia in 2014 and now is increasingly replacing VCUGs in CHOP’s Department of Radiology.
References and Further Readings
Darge K. Voiding urosonography with ultrasound contrast agents for the diagnosis of vesicoureteric reflux in children. I. Procedure. Pediatr Radiol. 2008;38(1):40-53.
Darge K, Troeger, J. Vesicoureteral reflux grading in contrast-enhanced voiding urosonography. Eur J Radiol. 2002;43(2):122-128.
Papadopoulou F, Ntoulia A, Siomou E, Darge K. Contrast-enhanced voiding urosonography with intravesical administration of a second-generation ultrasound contrast agent for diagnosis of vesicoureteral reflux: prospective evaluation of contrast safety in 1 010 children. Pediatr Radiol. 2014;44(6):719-28.
Darge K. Voiding urosonography with US contrast agents for the diagnosis of vesicoureteric reflux in children. II. Comparison with radiological examinations. Pediatr Radiol. 2008;38(1):54-63; quiz 126-127.
Contact us
Department of Radiology